We are very excited to announce, Early registration for the SNP Alliance Fall Forum 2026 is now open!
The SNP Alliance membership covers the full spectrum of Special Needs Plans:
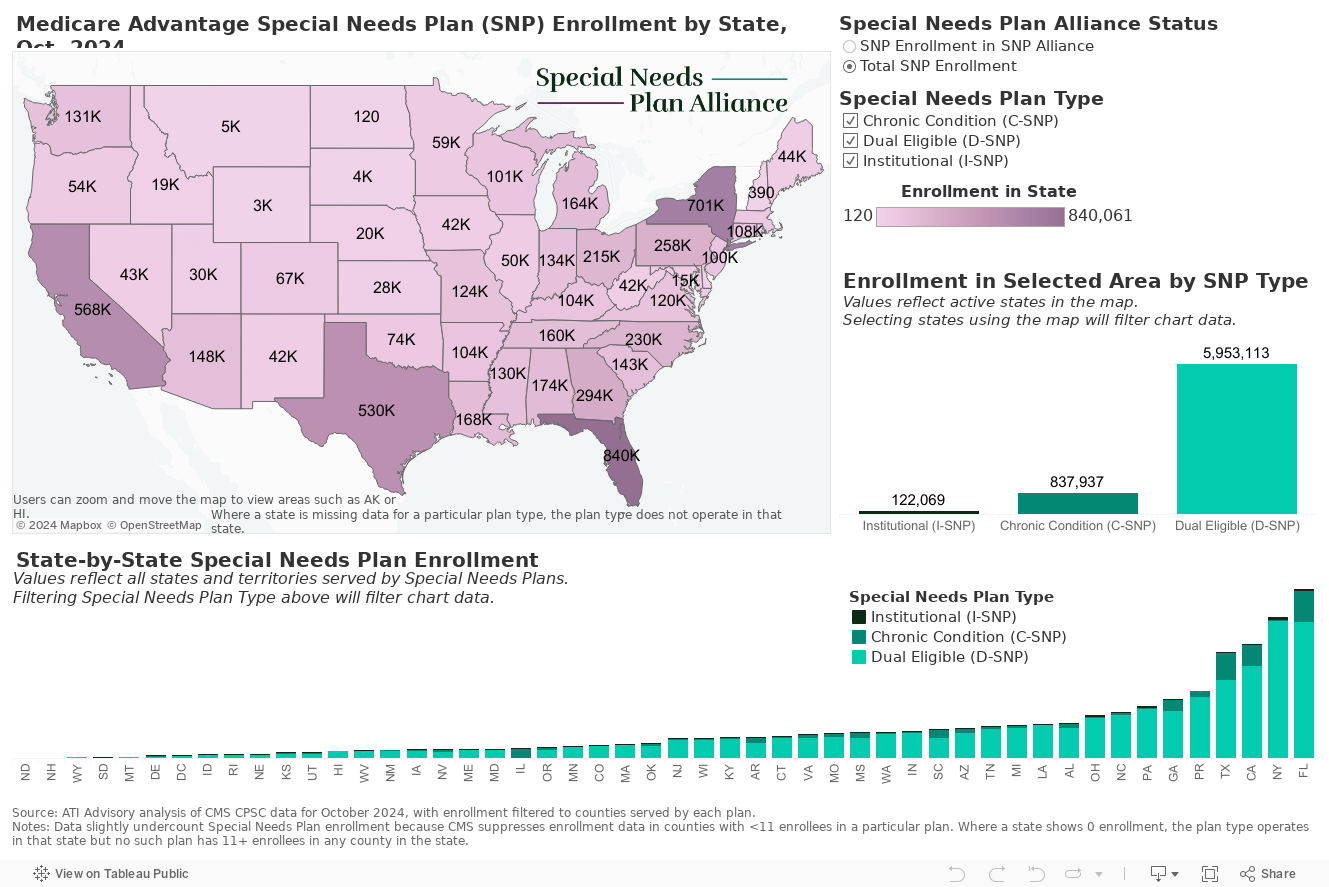
This includes Dual-Eligible SNPs (D-SNP) for beneficiaries eligible for both Medicare and Medicaid, Chronic or Disabling Condition Special Needs Plans (C-SNP) for individuals with multiple chronic conditions, and Institutional Special Needs Plans (I-SNP) for those living in nursing homes.
Some of our members also offer Medicare-Medicaid Plan demonstrations (MMP), which provide seamless operations and care for dually-eligible beneficiaries living in counties and states where these demonstrations are available.
Our members represent over two-thirds of the roughly 6 million Medicare beneficiaries currently enrolled in a SNP or MMP (as of April 2023).
Click below to learn more about the types of plans our members offer:
Dually Eligible SNPs
Dually Eligible SNPs specialize in care for persons dually eligible for Medicare and Medicaid.
FIDE and HIDE SNPs
Learn more about Fully and Highly Integrated Dual SNPs and new requirements from CMS.
Chronic Condition SNPs
Chronic Condition SNPs specialize in care of individuals with severe or disabling chronic conditions as specified by CMS.
Institutional SNPs
Institutional SNPs specialize in care of persons living in institutions or in the community with similar needs.
MMPs and CMMI Demos
Medicare-Medicaid plans and the growing list of delivery model demonstrations offered by CMS.

A very recent PHC enrollee, Jim, was hospitalized for failure to thrive and a serious infection. At the hospital, RN-CM learned John had not been taking his Antiretroviral medications and, because of this, was highly susceptible to catastrophic opportunistic infections, opportunistic cancers and death. After inpatient stabilization, the RN-CM worked to ensure smooth transition to an appropriate skilled nursing facility and then home. While at the Skilled Nursing Facility, Jim’s Plan of Care (POC) was updated. As part of this process, the RN-CM learned Jim was frustrated with the array of pills, multiple physicians’ offices and poor physician office communication.
With RN-CM support, Jim began taking his meds and streamlined his primary care physician (PCP) and other physician visits. During a routine visit, PCP detected a second infection. PCP contacted RN-CM to request assistance with an Emergency Department visit. RN-CM met Jim at the ED and coordinated a telehealth meeting between PCP and ED. With this clear communication, Jim was successfully treated with an appropriate IV antibiotic to target the infection and avoided an inpatient admission. Since this challenge, Jim continues to engage with the RN-CM and actively participates in his POC.